Mental Health Care Plans and Medicare Rebates for Psychology
If you are thinking about seeing a psychologist, or you are already a client, you may be able to claim a Medicare rebate for some of your sessions. This usually requires a referral from your General Practitioner under a Mental Health Treatment Plan, often still called a Mental Health Care Plan or MHCP. (1)
A Mental Health Care Plan does not make psychology sessions automatically free. It allows eligible clients to receive a Medicare rebate, which reduces the out-of-pocket expenses associated with therapy. At this practice, the session fee is higher than the Medicare rebate, so there will usually be a gap payment after Medicare has paid its rebate. (1)
This page explains how Mental Health Care Plans work, what Medicare currently contributes, and what changed from 1 July 2026.
What is a Mental Health Care Plan?
A Mental Health Care Plan is a plan prepared by your GP or another eligible medical practitioner. It is used when you have a diagnosed mental health condition and your doctor believes psychological treatment may be helpful. (1)
The plan usually includes your current concerns, treatment goals, referral details, and a review process. It may be used for concerns such as anxiety, depression, trauma-related symptoms, stress, adjustment difficulties, obsessive-compulsive symptoms, and other mental health conditions.
The formal Medicare term is now Mental Health Treatment Plan, but many people still know it as a Mental Health Care Plan.
What is Better Access to Mental Health Care?
Better Access to Mental Health Care is the Medicare initiative that allows eligible people to claim rebates for selected mental health treatment services. These services may be provided by eligible clinical psychologists, registered psychologists, General Practitioners, prescribed medical practitioners, social workers and occupational therapists. (2)
For psychology clients, Better Access is the program that usually applies when you bring a Mental Health Treatment Plan and referral from your GP.
How many psychology sessions can I claim through Medicare?
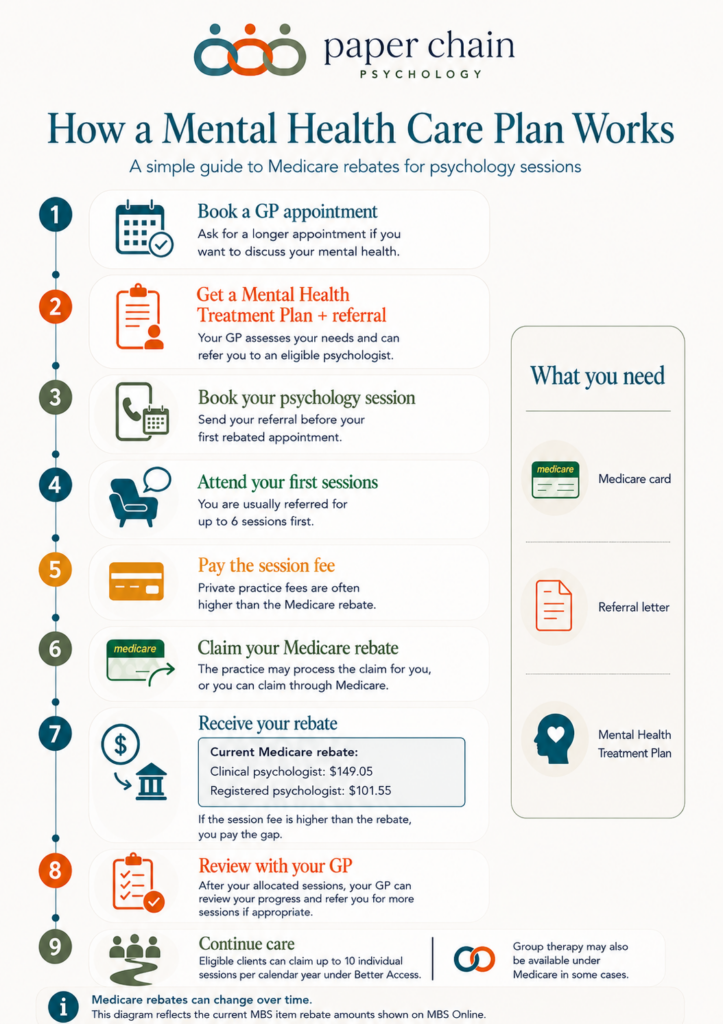
Under Better Access, eligible clients can claim Medicare rebates for up to 10 individual mental health treatment sessions per calendar year. The calendar year runs from 1 January to 31 December. (2)
Your GP will usually refer you for up to 6 sessions first. After those sessions, your GP can review your progress and decide whether further sessions are clinically appropriate. If so, you may be referred for additional sessions, up to the annual Medicare limit. (1)
You can continue therapy beyond the Medicare-rebated sessions if you choose, but Medicare will not rebate more than the annual limit under Better Access.
What about Group Therapy?
Better Access may also allow eligible clients to claim rebates for up to 10 group therapy mental health treatment services per calendar year. (2) Group Therapy is separate from individual therapy and is not the same as family therapy or couples therapy.
Not all psychology practices offer Group Therapy. If it is clinically relevant, your psychologist can discuss whether a group program may be suitable for your goals and circumstances.
Medicare rebate amounts from 1 July 2026
Medicare rebates changed from 1 July 2026 due to annual Medicare Benefits Schedule indexation. MBS Online published a 2.6% indexation factor for 1 July 2026. (3)
For a standard session of at least 50 minutes, the key rebates from 1 July 2026 are:
| Provider type | Common MBS item | Medicare rebate from 1 July 2026 |
|---|---|---|
| Clinical psychologist | 80010 | $149.05 |
| Registered psychologist | 80110 | $101.55 |
These figures are Medicare rebate amounts, not the full session fee. Psychologists set their own fees, and many private psychology practices charge more than the Medicare rebate. (1)
What does this mean for your out-of-pocket expenses?
Your out-of-pocket expense is the difference between the session fee and the Medicare rebate.
For example, if the session fee is higher than the rebate, you pay the full session fee at the time of your appointment and then receive the Medicare rebate back, provided you have a valid referral and have not exceeded your annual session limit.
This means a Mental Health Care Plan can make therapy more affordable, but it does not usually remove the cost completely. If you would like to understand your expected out-of-pocket cost, ask the practice about:
- the full session fee
- the Medicare item number used
- the rebate that applies
- whether the claim can be processed for you after payment
How do I get a Mental Health Care Plan?
To access Medicare rebates, book an appointment with your GP and explain that you would like to discuss your mental health and whether a Mental Health Treatment Plan is appropriate.
It is a good idea to book a longer GP appointment, as your General Practitioner will need time to assess your symptoms, discuss your history, and prepare the plan if you are eligible.
You can also ask your GP to address the referral letter to a specific psychologist or practice. Please bring or send your referral letter before your first rebated session, as Medicare rules require the referral to be in place for the rebate to apply. (4)
What should I bring to my first appointment?
Before your first Medicare-rebated psychology session, please make sure the practice has:
- your Mental Health Treatment Plan, if available
- your referral letter
- your Medicare card details
- any relevant information from your GP, psychiatrist, paediatrician or other treating health professional
Your Medicare Card is needed for Medicare claiming. If the practice can process your Medicare claim electronically, Medicare can usually pay the rebate into your registered bank account after the claim is processed. (5)
Do I need a new plan every year?
Usually, no. A Mental Health Treatment Plan does not automatically expire. However, you do need a valid referral for the sessions you are claiming. (4)
If you have unused sessions from a previous referral, they may still be usable, but any sessions claimed in the new calendar year count toward that year’s Medicare limit. Once you have used the sessions covered by your referral, you will need to return to your GP for a review or further referral if more Medicare-rebated sessions are appropriate.
A new Mental Health Treatment Plan is generally only needed if there has been a significant change in your mental health, or if your previous plan cannot be accessed.
Can I claim Medicare for online psychology sessions?
In many cases, yes. Medicare rebates may be available for eligible telehealth psychology sessions, including video consultations, where the usual Better Access requirements are met. (2)
Telehealth can be helpful if you live outside the local area, have mobility or transport difficulties, are unwell, or prefer online therapy. Your psychologist can discuss whether telehealth is clinically appropriate for your circumstances.
Can I use Medicare and private health insurance together?
You generally need to choose either Medicare or private health insurance for a session. Private health insurance usually cannot be used to “top up” the Medicare rebate for the same appointment. (4)
If you have used all of your Medicare-rebated sessions for the year, you may be able to claim future sessions through private health insurance, depending on your policy. Check directly with your health fund, as cover and rebate amounts vary.
How do I receive the Medicare rebate?
Many practices can process your Medicare claim electronically after you pay for your session. If this is available, Medicare usually pays the rebate into your registered bank account.
If the practice does not process the claim for you, you can claim through your Medicare online account linked to myGov, the myGov app, by mail, or at a Services Australia service centre. (5)
Does the Medicare Safety Net help?
If you have high out-of-pocket medical costs in a calendar year, the Medicare Safety Net may help you receive a higher benefit for some out-of-hospital services once you reach the relevant threshold. (6)
The session fee itself does not change, but your Medicare rebate may increase after you reach the threshold. Services Australia calculates Safety Net thresholds each calendar year. Couples and families may be able to register as a family so their eligible out-of-pocket costs are combined.
Key things to know before your first appointment
Before your first Medicare-rebated psychology session, it helps to confirm:
- you have a valid Mental Health Treatment Plan and referral letter
- the referral is addressed to the psychologist or practice
- the number of sessions included in the referral
- the full session fee
- the Medicare rebate that applies from 1 July 2026
- your expected out-of-pocket expenses
- whether the practice can process your Medicare claim after payment
- that your Medicare Card details are up to date
FAQs
Are Mental Health Care Plans covered by Medicare?
The GP appointment to prepare a Mental Health Treatment Plan may be covered partly or fully by Medicare, depending on your GP’s billing policy. The plan can then allow you to claim Medicare rebates for eligible psychology sessions. (1)
Can I get 10 free psychology sessions?
Not usually. Medicare may rebate up to 10 individual sessions per calendar year, but sessions are only free if the psychologist bulk bills. At many private psychology practices, including practices where fees are higher than the Medicare rebate, there is an out-of-pocket cost. (1)
What is the current Medicare rebate for psychology?
From 1 July 2026, the Medicare rebate for a standard 50-minute session is $149.05 with a clinical psychologist under item 80010, and $101.55 with a registered psychologist under item 80110. (3)
Can I see a psychologist without a Mental Health Care Plan?
Yes. You can see a psychologist privately without a Mental Health Care Plan or referral. However, you usually need a valid referral and plan to claim Medicare rebates under Better Access. (2)
Can my GP refer me to a specific psychologist?
Yes. You can ask your GP to refer you to a specific psychologist or psychology practice. The psychologist must be eligible to provide Medicare-rebated services for a rebate to apply. (4)
References
- Services Australia — Mental health care and Medicare
https://www.servicesaustralia.gov.au/mental-health-care-and-medicare?context=60092 - Australian Government Department of Health, Disability and Ageing — Better Access initiative
https://www.health.gov.au/our-work/better-access-initiative - MBS Online — July 2026 MBS changes; Item 80010; Item 80110
https://www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/news-260701
https://www9.health.gov.au/mbs/fullDisplay.cfm?q=80010&type=item
https://www9.health.gov.au/mbs/fullDisplay.cfm?q=80110&type=item - Services Australia — MBS billing rules for mental health services
https://www.servicesaustralia.gov.au/mbs-billing-rules-for-mental-health-services?context=20 - Services Australia — Medicare claims
https://www.servicesaustralia.gov.au/medicare-claims?context=60092 - Australian Government Department of Health, Disability and Ageing — Medicare Safety Nets
https://www.health.gov.au/topics/medicare/about/safety-nets